kottke.org posts about medicine
Great Ormond Street Hospital for Children (GOSH) in London improved their surgery-to-ICU handoff process by observing how Ferrari’s F1 team handled pit stops.
GOSH doctors visited and observed the pit crew handoff in Italy. While visiting the Formula One pit crew the GOSH doctors became interested in the way they addressed possible failure. The crew sat around a big table analyzing and reanalyzing, asking, “What could go wrong?” and “What are we going to do if it does go wrong?” and “How important is it if it goes wrong?” Everyone’s ideas were given equal weight until the group ranked them using the failure modes and effect analysis (FMEA).
This anticipatory planning made the pit crew more prepared than the medical team whose strategy tended to be waiting until something went wrong to work out what they should have done. Observing the pit crew, the GOSH doctors noted the value of process mapping, process description, and trying to work out what people’s tasks should be. They learned the keys to a successful pit stop:
– The routine in the pit stop is taken seriously
– What happens in the pit stop is predictable so problems can be anticipated and procedures can be standardized
– Crews practice those procedures until they can perform them perfectly
– Everyone knows their job, but one person is always in charge
Among their findings that led to improvement:
While the main theme changes were more sophisticated procedures and better choreographed teamwork, another aspect of the Formula One handover process easily transferred to the hospital setting. The lollipop man is the one who waves the car in and coordinates the pit stop. He maintains overall situation awareness during the pit stop. In the old hospital handover there was no one like the lollipop man so it was unclear who was in charge. Under the new handover process, the anesthetist was given overall responsibility for coordinating the team until it was transferred to the intensivist at the termination of the handover. These same two individuals were charged with the responsibility of periodically stepping back to look at the big picture and to make safety checks of the handover.
According to this video about the hospital’s study, they were able to reduce the number of errors in the handover by 66%.
(thx, meg)
In a letter to the Times of London, Dr. Michael Baum tells how a line in Arcadia by Tom Stoppard sparked an idea which resulted in adjuvant systemic chemotherapy, a therapy Baum helped pioneer which greatly increased the survivability of breast cancer.
Sir, In 1993 my wife and I went to see the first production of Arcadia by Tom Stoppard (obituary, Dec 1), and in the interval I experienced a Damascene conversion. As a clinical scientist I was trying to understand the enigma of the behaviour of breast cancer, the assumption being that it grew in a linear trajectory spitting off metastases on its way. In the first act of Arcadia, Thomasina asks her tutor, Septimus: “If there is an equation for a curve like a bell, there must be an equation for one like a bluebell, and if a bluebell, why not a rose?” With that Stoppard explains chaos theory, which better explains the behaviour of breast cancer. At the point of diagnosis, the cancer must have already scattered cancer cells into the circulation that nest latent in distant organs. The consequence of that hypothesis was the birth of “adjuvant systemic chemotherapy”, and rapidly we saw a striking fall of the curve that illustrated patients’ survival.
Stoppard never learnt how many lives he saved by writing Arcadia.
Michael Baum
Professor emeritus of surgery; visiting professor of medical humanities, UCL
Certainly drives home the value of a robust and diverse culture of humanities in contradiction to the current backlash. (via @harrywallop.co.uk)
It’s not often that a movie trailer makes you cry — but this one might.1
Come See Me in the Good Light is a documentary film about poets Andrea Gibson and Megan Falley facing a cancer diagnosis that took Gibson’s life earlier this year.
This is the beginning of a nightmare, I thought. But stay with me, y’all, because my story is one about happiness, being easier to find, once we realize we do not have forever to find it.
Falley’s letter published just after Gibson’s death will give you a sense of the spirit of the film & the two humans at the center of it:
A couple years ago, Andrea said, “Whenever I leave this world, whether it’s sixty years from now, I wouldn’t want anyone to say I lost some battle. I’ll be a winner that day.”
Whatever beast of emotion bucks or whimpers through you right now, I hope you can hold that line beside it: Andrea didn’t lose anything. If you had been here in our home during the three days of their dying — if you’d seen dozens of friends drift in to help, to say goodbye, to say thank you, to kiss their perfect face, if you’d felt the love that floored every hospice nurse — you would have agreed. Andrea won.
The film is set to premiere Nov 14 on Apple TV.
Dr. Katelyn Jetelina (aka Your Local Epidemiologist) has a frustrating update on how Covid vaccines are probably going to work this fall under the ideologically corrupt Trump regime.
The FDA is expected to license the Covid-19 vaccine. Word is that the label will be restricted to adults 65+ and people at high risk.
The Vaccine Integrity Project and professional organizations likely won’t align with RFK Jr.’s FDA license, which will cause confusion.
If you’re younger than 65 and don’t have a chronic condition, could you still get it after the label change?
Yes, but it will be complicated. While a provider could prescribe it off-label, in practice, it’s likely that most people won’t be able to access it that way.
Jetelina continues:
If you’re under 65 and not high risk, the window to get a Covid-19 vaccine is right now — before the FDA label changes. Once it happens, access will be limited immediately (if it isn’t already). CVS is no longer booking appointments. As far as we know, Walgreens and local pharmacies still are.
That was as of Monday — no idea if that’s still the case. And of course, because this is the United States, insurance will probably be a mess too:
Recommendations from these two organizations are really important for insurers. The hope is they see them and cover all vaccines, regardless of what RFK does. It also provides extra information to physicians who will prescribe off-label if RFK Jr’s FDA changes the label (as expected) this Friday.
We will not know if any of these recommendations affect insurance coverage until insurance companies confirm coverage.
[insert a lot of profanity here; seriously, this makes me so incandescently mad that if I wrote anything more it would contain every fucking swear word I know and then some]
Sources: Aug 18 thread on Bluesky, Aug 20 thread on Bluesky, Aug 18 newsletter.
This is a great data-driven short documentary by Neil Halloran about how smallpox was eradicated from the face of the Earth. And what it took was humanity, through the use of science & humanitarianism, answering its own plea for something to be done about it.
Some philosophers believe there was a secondary humanitarian revolution that followed the scientific revolution. And I note this because the eradication of smallpox also had these two phases. The scientific breakthroughs of inoculation and the vaccine allowed many countries to become virtually smallpox-free — but not all countries. In fact, those 300 to 500 million deaths in the 20th century? They came well after the vaccine had been discovered. So clearly, for much of the world, something more was needed than medical innovation. And fortunately there’s reason to think that these two types of progress might be connected.
Part of being a human is contemplating why some of us get so sick. It’s a practical question and it’s more than that. As we learned about disease, the theory goes that we began to think a little differently about those who fell ill — to see that their suffering truly wasn’t meant to be. We stepped away from thinking it was up to a higher power and into the belief that, well, it was up to us.
See also How smallpox claimed its final victim (I’d never heard this story before watching Halloran’s video), How Children Took the Smallpox Vaccine Around the World, and No One Knows What’s Inside the Smallpox Vaccine.
I loved this short thread from Andrew Miller about how his pediatrician wife helps parents who are skeptical of vaccinating their children change their minds.
So my wife is a pediatrician and works in some hospitals with high vaccine and intervention hesitation (suburban ones). She has found *tremendous* success by just letting the families know she will have to document the higher risk of specific, and often fatal illness, in the chart of their child.
She explains that if their child goes to the ER, the ER might not think to ask about routine newborn care that the parents opted out of, so by putting it in the chart she might be saving the child from this very specific thing. But just as important it makes it feel REAL to the parents.
She identifies and describes the specific thing that their child is now more likely to die from. In detail, including symptoms to watch out for. It’s not abstract. It’s visceral.
Premiering this Friday (Nov 22) on FX is a short documentary from The New York Times called Weight of the World about GLP-1 drugs. Here’s the synopsis:
As GLP-1 drugs like Ozempic soar in popularity for weight loss, this film follows three people on their own GLP-1 journeys and explores how decades of diet culture and society’s relentless pursuit of thinness paved the way for their rise.
The doc features Roxane Gay & Tressie McMillan Cottom and will will be available on Hulu on Nov 23.
I’d missed that Time magazine is naming a “Kid of the Year” now and this year’s recipient is 15-year-old scientist Heman Bekele, who has developed a soap that could treat and even prevent skin cancer.
A few years ago, he read about imiquimod, a drug that, among other uses, is approved to fight one form of skin cancer and has shown promise against several more. Typically, imiquimod, which can help destroy tumors and usually comes in the form of a cream, is prescribed as a front-line drug as part of a broader cancer treatment plan, but Heman wondered if it could be made available more easily to people in the earliest stages of the disease. A bar of soap, he reckoned, might be just the delivery system for such a lifesaving drug, not just because it was simple, but because it would be a lot more affordable than the $40,000 it typically costs for skin-cancer treatment.
“What is one thing that is an internationally impactful idea, something that everyone can use, [regardless of] socioeconomic class?” Heman recalls thinking. “Almost everyone uses soap and water for cleaning. So soap would probably be the best option.”
Kurzgesagt explores what happens when a virus or bacteria enters a human body and the essential role fever plays in helping your body fight off disease.
Fever feels bad. So we take medication to suppress it — but is this a good idea? It turns out fever is one of the oldest defenses against disease. What exactly is a fever, and how does it make your immune defense stronger? Should you take a pill to combat it?
We often mistake fever for the disease…it’s actually part of the cure. When my kids were young, I vividly remember our laissez-faire French pediatrician urging us not to give them medication to get rid of their fevers because that was the body fighting back and doing useful work — unless their temps got too high of course.
This piece by Lydia Polgreen on The Strange Report Fueling the War on Trans Kids is so good — straightforward and informative, especially when compared to the incoherent nonsense that the NY Times has run about trans people over the past few years. The piece is about, in Polgreen’s words, “the sneaky effort to use what looks like science to justify broad intrusions in our personal freedom”.
I usually don’t do this, but I’ve excerpted the article’s conclusion here because it just gets right to the heart of an urgent concern: the freedom to control our own bodies.
Imagine that your health care required objective justification, if access to birth control or erectile dysfunction medications required proving that you were having monogamous sex, or good sex, or sex at all. Or if fertility care was provided only if you could prove that becoming a parent would make you happy, or you would be a good parent. Or that abortion would be available only if you could prove that it would improve your life.
In a free society we agree that these are private matters, decided by individuals and their families, with the support of doctors using mainstream medical science as a guide, even when they involve children. We invite politicians and judges into them at great peril to our freedom.
I encourage you to read the whole thing — it’s interesting throughout.
John Green recently teamed up with Kurzgesagt for a video on one of the world’s deadliest diseases: tuberculosis.
The white death has haunted humanity like no other disease following us for thousands, maybe millions of years. In the last 200 years it killed a billion people — way more than all wars and natural disasters combined. Even today it’s the infectious disease with the highest kill count.
The maddening bit is that tuberculosis is curable…it’s just that the cure is not equally distributed around the world.
4,000 people died of tuberculosis yesterday, and we simply don’t have to accept a world where so many of us still die of a disease we know how to cure. The White Death has been with us for millions of years. It is time to continue our journey without it.
Contractions is a powerful short film by Lynne Sachs about a former abortion clinic in Tennessee, a state where abortion is almost completely banned.
If I can’t make the same medical decisions about my body with autonomy, I’m a second-class citizen. And you basically, as a physician, had to start counseling your patients from a legal perspective and not a medical perspective.
In the film, we hear from an anonymous woman who is a volunteer driver for patients; she drives them nine hours RT to get abortion care in Illinois:
I had on patient, a young woman of color, and she said to me, “You know, this is really crazy. I kind of feel like I’m on the new Underground Railroad.”
This makes me so fucking angry. If you’d like, you can join me in rage-donating to CHOICES Center for Reproductive Health (the clinic featured in the film, now located in Illinois), ARC Southeast (providing practical support for Southerns seeking abortions), and Midwest Access Coalition (a practical abortion fund that helps people traveling to, from, and within the Midwest to access a safe, legal abortion).
Many Patients Don’t Survive End-Stage Poverty by Dr. Lindsay Ryan is a great/upsetting piece about how the poverty many Americans are subjected to in America is killing them. Many people die here in the world’s richest country not because they are sick but because they are poor and our systems of government, justice, business, and health care don’t do enough to help them (or, more cynically and perhaps truthfully, actively work against helping them).
This is one of those pieces where I want to quote every single paragraph, but I’ll start with this one (bold mine):
Safety-net hospitals and clinics care for a population heavily skewed toward the poor, recent immigrants and people of color. The budgets of these places are forever tight. And anyone who works in them could tell you that illness in our patients isn’t just a biological phenomenon. It’s the manifestation of social inequality in people’s bodies.
I have not been able to stop thinking about this phrase since I read it: “Illness in our patients isn’t just a biological phenomenon. It’s the manifestation of social inequality in people’s bodies.”
Medical textbooks usually don’t discuss fixing your patient’s housing. They seldom include making sure your patient has enough food and some way to get to a clinic. But textbooks miss what my med students don’t: that people die for lack of these basics.
People struggle to keep wounds clean. Their medications get stolen. They sicken from poor diet, undervaccination and repeated psychological trauma. Forced to focus on short-term survival and often lacking cellphones, they miss appointments for everything from Pap smears to chemotherapy. They fall ill in myriad ways — and fall through the cracks in just as many.
You should read the whole thing yourself (NY Times gift link). Her argument about the need to expand/shift the definition of what healthcare is (e.g. housing is healthcare) reminds me of this more progressive idea of freedom.
In this Crash Course video, author and “TB-hater” John Green takes a deep dive into tuberculosis.
This is the story of the deadliest infectious disease of all time. It’s been with us for 3 million years, since before humans were homo sapiens. We have evidence of it in the mummies of ancient Egypt, and it’s mentioned in the Hebrew Bible.
We’ve made extraordinary medical advances. Vaccines, antibiotics, and clean water have saved millions of lives. And yet despite that, in 2022, this disease killed more people than malaria, typhoid, cholera, homicide, and war…combined.
It has gone by many names. In ancient China, it was known as huaifu, meaning “destroyed palace.” In ancient Hebrew, “schachepheth,” meaning wasting away. The 19th-century term: “consumption,” for the way it seemed to consume the body. Today, we call it tuberculosis.
From The Economist on the occasion of the award of the Nobel Prize for Medicine to Katalin Karikó and Drew Weissman for their work that led to the development of the Covid-19 mRNA vaccines, a lovely short appreciation of vaccines.
The World Health Organisation (WHO) says that vaccines have saved more from death than any other medical invention. It is a hard claim to gainsay. Vaccines protect people from disease cheaply, reliably and in remarkable numbers. And their capacity to do so continues to grow. In 2021 the who approved a first vaccine against malaria; this week it approved a second.
Vaccines are not only immensely useful; they also embody something beautifully human in their combination of care and communication. Vaccines do not trick the immune system, as is sometimes said; they educate and train it. As a resource of good public health, they allow doctors to whisper words of warning into the cells of their patients. In an age short of trust, this intimacy between government policy and an individual’s immune system is easily misconstrued as a threat. But vaccines are not conspiracies or tools of control: they are molecular loving-kindness.
The WHO says that vaccines currently prevent 4-5 million deaths per year. The CDC points to a paper that says that more than 50 million death can be prevented between 2021 and 2030. Vaccination is nothing short of a scientific miracle. (via eric topol)
Madeline Miller (Circe, Song of Achilles) got sick in February 2020 with what turned out to be Covid, which then turned into Long Covid. It has profoundly affected her life (gift link).
I reached out to doctors. One told me I was “deconditioned” and needed to exercise more. But my usual jog left me doubled over, and when I tried to lift weights, I ended up in the ER with chest pains and tachycardia. My tests were normal, which alarmed me further. How could they be normal? Every morning, I woke breathless, leaden, utterly depleted.
Worst of all, I couldn’t concentrate enough to compose sentences. Writing had been my haven since I was 6. Now, it was my family’s livelihood. I kept looking through my pre-covid novel drafts, desperately trying to prod my sticky, limp brain forward. But I was too tired to answer email, let alone grapple with my book.
When people asked how I was, I gave an airy answer. Inside, I was in a cold sweat. My whole future was dropping away. Looking at old photos, I was overwhelmed with grief and bitterness. I didn’t recognize myself. On my best days, I was 30 percent of that person.
I turned to the internet and discovered others with similar experiences. In fact, my symptoms were textbook — a textbook being written in real time by “first wavers” like me, comparing notes and giving our condition a name: long covid.
Even if Miller were physically able to get back to some semblance of “normal life”, the current policies and attitudes w/r/t Covid make it next to impossible.
Despite the crystal-clear science on the damage covid-19 does to our bodies, medical settings have dropped mask requirements, so patients now gamble their health to receive care. Those of us who are high-risk or immunocompromised, or who just don’t want to roll the dice on death and misery, have not only been left behind — we’re being actively mocked and pathologized.
I’ve personally been ridiculed, heckled and coughed on for wearing my N95. Acquaintances who were understanding in the beginning are now irritated, even offended. One demanded: How long are you going to do this? As if trying to avoid covid was an attack on her, rather than an attempt to keep myself from sliding further into an abyss that threatens to swallow my family.
I cannot remember where I read this (it was likely more than a year ago), but it would be more accurate/helpful if we thought of the disease caused by the SARS-CoV-2 virus as a chronic vascular disease (aka Long Covid) that often comes with short-term symptoms and acute, life-threatening effects instead of the other way around.
Using the metaphor of a cancerous tumor as an unruly village, Kurzgesagt explains how cancer develops in the human body, how the body fights against it, and how, sometimes, the cancer develops into something unmanageable.
In a sense this tiny tumor is like a rogue town. Imagine a group of rebels in Brooklyn decided that they were no longer part of New York but started a new settlement called Tumor Town, which happens to occupy the same space. The new city wants to grow, so it orders tons of steel beams, cement and drywall. New buildings follow no logic, are badly planned, ugly and dangerously crooked. They are built right in the middle of streets, on top of playgrounds and on existing infrastructure. The old neighborhood is torn down or overbuilt to make room for new stuff. Many of the former residents are trapped in the middle of it and begin to starve. This goes on for a while until the smell of death finally attracts attention. Building inspectors and police show up.
Last week, popular YouTuber, author, and science communicator Hank Green announced that he had cancer (very treatable Hodgkin’s lymphoma). His video announcement was part of a series of back-and-forth videos he does with his brother John Green, popular YouTuber and novelist. John replied to Hank’s video with a short one of his own, noting that humor is one way that people deal with grief but also a way in which we can accompany people through tough times.
To work, the humor has to feel like love rather than judgment, like inclusion rather than stigma, and like celebration rather than dismissal. And that’s a tough balance. Sometimes well-intentioned people, including me, get it wrong. And it also depends on, like, who’s saying it and the context.
Good luck and my warmest thoughts to the Greens and their family as they navigate this difficult time. And, you know, fuck cancer.
Writing for The Atlantic, Sarah Zhang details how some people taking Ozempic for weight loss are reporting that the drug has also curbed their addictive impulses (to drink, to shop, to smoke).
Earlier this year, she began taking semaglutide, also known as Wegovy, after being prescribed the drug for weight loss. (Colloquially, it is often referred to as Ozempic, though that is technically just the brand name for semaglutide that is marketed for diabetes treatment.) Her food thoughts quieted down. She lost weight. But most surprisingly, she walked out of Target one day and realized her cart contained only the four things she came to buy. “I’ve never done that before,” she said. The desire to shop had slipped away. The desire to drink, extinguished once, did not rush in as a replacement either. For the first time — perhaps the first time in her whole life — all of her cravings and impulses were gone. It was like a switch had flipped in her brain.
Not everyone experiences these effects, but there’s enough anecdotal evidence at this point that scientists are interested and investigating.
From The Atlantic, 23 Pandemic Decisions That Actually Went Right, the result of interviews with more than a dozen pandemic experts.
17. Basic research spending matters. The COVID vaccines wouldn’t have been ready for the public nearly as quickly without a number of existing advances in immunology, Anthony Fauci, the former head of the National Institute of Allergy and Infectious Diseases, told us. Scientists had known for years that mRNA had immense potential as a delivery platform for vaccines, but before SARS-CoV-2 appeared, they hadn’t had quite the means or urgency to move the shots to market. And research into vaccines against other viruses, such as RSV and MERS, had already offered hints about the sorts of genetic modifications that might be needed to stabilize the coronavirus’s spike protein into a form that would marshal a strong, lasting immune response.
From Kurzgesagt, an accessible explanation of what happens to the human body when you get sick.
Your brain activates sickness behavior and reorganizes your body’s priorities to defense. The first thing you notice is that your energy level drops and you get sleepy. You feel apathetic, often anxious or down and you lose your appetite. Your sensitivity to pain is heightened and you seek out rest. All of this serves to save your energy and reroute it into your immune response.
They also reveal the best way to boost your immune system to protect yourself against disease. I don’t want to spoil it but it’s vaccines. Vaccines are one of the best things humans have ever invented.
In the last several months, semaglutide, a drug originally developed to help manage type 2 diabetes, has been in the news for its “breakthrough” weight loss abilities. This video from Vox is a good overview of what the drug does and the interest & controversy around it.
Both Ozempic and Wegovy, Ozempic’s counterpart approved specifically for weight loss by the FDA, are brand names of a drug called semaglutide. Semaglutide is one of several drugs that mimics a crucial digestive hormone called glucagon-like peptide 1, or GLP-1. It amplifies a process our bodies perform naturally.
GLP-1 is released in our intestines when we eat, and there are receptors for the hormone in cells all over the body. In the pancreas, GLP-1 promotes the production of insulin and suppresses the production of glucagon. This helps insulin-resistant bodies, like those with type 2 diabetes or obesity, manage blood sugar levels. In the stomach, GLP-1 slows gastric emptying, extending the feeling of being full. In the brain, GLP-1 suppresses appetite, which also promotes satiety and curbs hunger, so we eat less.
Jia Tolentino wrote a long piece about semaglutide for the New Yorker this week: Will Ozempic Change How We Think About Being Fat and Being Thin?
But, as I kept reminding Ozempic-curious friends, these medications were designed for chronic conditions, obesity and diabetes. For people who are dealing with those conditions, Ozempic appears to create a path toward a healthy relationship to food. For those who aren’t, it might function more like an injectable eating disorder. As the side effects make clear, it’s not a casual thing to drastically alter your body’s metabolic process, and there is no large-scale data about the safety of these drugs when taken by people who are mainly interested in treating another chronic condition, the desire to be thin.
Julia Belluz wrote a piece for Vox on Obesity in the age of Ozempic and Eric Topol wrote about The New Obesity Breakthrough Drugs.
Update: In the shuffle of the last few months, I’d missed reading Paul Ford’s piece about “the post-hunger age”, A New Drug Switched Off My Appetite. What’s Left?
I can see my anxiety mirrored in the wave of reactions starting to appear — op-eds, TV segments, people explaining why it’s good, actually, that the vast majority of those using this drug lose a quarter of their body weight. On social media, fat activists are pointing out that our lives were worthy even without this drug. The wave of opinion will not crest for years.
And that’s fair because this is new — not just the drug, but the idea of the drug. There’s no API or software to download, but this is nonetheless a technology that will reorder society. I have been the living embodiment of the deadly sin of gluttony, judged as greedy and weak since I was 10 years old-and now the sin is washed away. Baptism by injection. But I have no more virtue than I did a few months ago. I just prefer broccoli to gloopy chicken. Is this who I am?
Even outside the context of drugs, I find the tension between accepting who you are versus trying to change some behavior you find unappealing is challenging to navigate — it’s something that comes up in therapy a lot. (thx, anil)
Well, this is potentially a huge deal:
In a potential game changer for the treatment of superbugs, a new class of antibiotics was developed that cured mice infected with bacteria deemed nearly “untreatable” in humans — and resistance to the drug was virtually undetectable.
Developed by a research team of UC Santa Barbara scientists, the study was published in the journal eBioMedicine. The drug works by disrupting many bacterial functions simultaneously — which may explain how it killed every pathogen tested and why low-level of bacterial resistance was observed after prolonged drug exposure.
Huge if true, etc. What really caught my attention is how they discovered this in the first place…they were working on a way to charge cell phones:
The discovery was serendipitous. The U.S. Army had a pressing need to charge cell phones while in the field — essential for soldier survival. Because bacteria are miniature power plants, compounds were designed by Bazan’s group to harness bacterial energy as a “‘microbial”’ battery. Later the idea arose to re-purpose these compounds as potential antibiotics.
“When asked to determine if the chemical compounds could serve as antibiotics, we thought they would be highly toxic to human cells similar to bleach,” said Mahan, the project lead investigator. “Most were toxic — but one was not — and it could kill every bacterial pathogen we tested.”
Here’s the original paper if you’d like to take a look.
Zeynep Tufekci on the H5N1 strain of the avian influenza, which is showing some recent signs of spreading in mammals.
Bird flu — known more formally as avian influenza — has long hovered on the horizons of scientists’ fears. This pathogen, especially the H5N1 strain, hasn’t often infected humans, but when it has, 56 percent of those known to have contracted it have died. Its inability to spread easily, if at all, from one person to another has kept it from causing a pandemic.
But things are changing. The virus, which has long caused outbreaks among poultry, is infecting more and more migratory birds, allowing it to spread more widely, even to various mammals, raising the risk that a new variant could spread to and among people.
Alarmingly, it was recently reported that a mutant H5N1 strain was not only infecting minks at a fur farm in Spain but also most likely spreading among them, unprecedented among mammals. Even worse, the mink’s upper respiratory tract is exceptionally well suited to act as a conduit to humans, Thomas Peacock, a virologist who has studied avian influenza, told me.
The three relevant facts here are: 56% of humans who’ve contracted H5N1 have died, there are signs of spreading among mammals, and that particular mammal is “exceptionally well suited” to pass viral infections along to humans. Tufekci, who attempted to sound the alarm relatively early-on about Covid-19, goes on to urge the world to action about H5N1, before it’s too late. Will we act? (No. The answer is no.)
*sigh*
You know, it’s a little shocking to read about a potential solution to the Fermi paradox on a random February Monday, but here we are.
Men in the US typically do not talk about or worry about birth control that much, to the detriment of the health and safety of women. In the spirit of trying to change that a little, I’m going to talk to you about my experience. About a decade ago, knowing that I did not want to have any more children, I had a vasectomy. And let me tell you, it’s been great. Quickly, here’s what a vasectomy is, via the Mayo Clinic:
Vasectomy is a form of male birth control that cuts the supply of sperm to your semen. It’s done by cutting and sealing the tubes that carry sperm. Vasectomy has a low risk of problems and can usually be performed in an outpatient setting under local anesthesia.
Whether you’re in a committed relationship or a more casual one, knowing that you’re rolling up to sexual encounters with the birth control handled is a really good feeling for everyone concerned.1 Women have typically (and unfairly) had to be the responsible ones about birth control, in large part because it’s ultimately their body, health, and well-being that’s on the line if a sexual act results in pregnancy, but there are benefits of birth control that accrue to both parties (and to society) and taking over that important responsibility from your sexual partner is way more than equitable.
(Here’s the part where I need to come clean: getting a vasectomy was not my idea. I had to be talked into it. It seemed scary and birth control was not something I thought about as much as I should have. I’m ashamed of this; I wish I’d been more proactive and taken more responsibility about it. Guys, we should be talking about and thinking about this shit just as much as women do! I hope you’ve figured this out earlier than I did. Ok, back to the matter at hand.)
Vasectomies are often covered by health insurance and are (somewhat) reversible. These issues can be legitimate dealbreakers for some people. Some folks cannot afford the cost of the procedure or can’t take the necessary time off of work to recover (heavy lifting is verboten for a few days afterwards). And if you get a vasectomy in your 20s for the purpose of 10-15 years of birth control before deciding to start a family, the lack of guarantee around reversal might be unappealing. Talk to your doctor, insurance company, and place of employment about these concerns!
Does the procedure hurt? This is a concern that many men have and the answer is yes: it hurts a little bit during and for a few days afterwards. For most people, you’re in and out in an hour or two, you ice your crotch, pop some Advil, take it easy for a few days, and you’re good to go.1 It’s a small price to pay and honestly if you don’t want to get a vasectomy because you’re worried about your balls aching for 48 hours, I’m going to suggest that you are a whiny little baby — and I’m telling you this as someone who is quite uncomfortable and sometimes faints during even routine medical procedures.
So, if you’re a sperm-producing person who has sex with people who can get pregnant and do not wish for pregnancy to occur, you should consider getting a vasectomy. It’s a minor procedure with few side effects that results in an almost iron-clad guarantee against unwanted pregnancy. At the very least, know that this is an option you have and that you can talk to your partner and doctor about it. Good luck!
Dr. Dipti S. Barot writing for HuffPost, My 11-Year-Old Patient Was Pregnant. Here’s What I Want You To Know About Being ‘Pro-Life.’ (Content warning: rape.)
Sophia is in her 20s now. I wonder how she has healed, how she has processed that trauma. Did she get to go to college? Has she been able to trust an intimate partner? Has she been pregnant on her own terms at the time of her choosing? Does she have a child? I can see her wide face and her soft smile in my mind’s eye and I know now, just as I knew then, that the decision to terminate Sophia’s pregnancy, supported by the ones who loved her the most, was a pro-life decision.
And:
I remember how tiny that clinic room felt. There was no room for politicians signing evil bills flanked by child props as old as Sophia, no room for Supreme Court justices who claim to value life while wondering aloud how pregnancy can be an undue burden. No room for those extraneous, unnecessary, useless others in that most intimate of spaces. Our clinic rooms will always be too small for anybody but providers and our patients.
From Lindsay Holiday, an engaging history of birth control, covering the ineffective and often dangerous methods used in the ancient world, the rhythm method, proto-condoms, actual condoms, Lysol (!!), and of course one of the modern world’s most impactful inventions, the hormonal birth control pill.
Through most of history pregnancy and childbirth were a very dangerous undertaking for women. In medieval Europe 1 in 3 women died in their child-bearing years and 1 in 4 children did not live to see their first birthday. Even when both mother and child survived the ordeal of birth women were not always able to provide for a child. And in most cultures pregnancy outside of wedlock was considered a great sin and often resulted in the shunning of the woman and child while the man often got away scot-free. It is no surprise therefore that women throughout history have been trying a wide variety of methods to prevent conception.
(via open culture)
In his newest piece for The Atlantic, Ed Yong explores why, despite more than 6 million official deaths worldwide and almost a million official deaths in the US, the toll of the pandemic isn’t provoking a massive social reckoning. This is a hell of an opening paragraph:
The United States reported more deaths from COVID-19 last Friday than deaths from Hurricane Katrina, more on any two recent weekdays than deaths during the 9/11 terrorist attacks, more last month than deaths from flu in a bad season, and more in two years than deaths from HIV during the four decades of the AIDS epidemic. At least 953,000 Americans have died from COVID, and the true toll is likely even higher because many deaths went uncounted. COVID is now the third leading cause of death in the U.S., after only heart disease and cancer, which are both catchall terms for many distinct diseases. The sheer scale of the tragedy strains the moral imagination. On May 24, 2020, as the United States passed 100,000 recorded deaths, The New York Times filled its front page with the names of the dead, describing their loss as “incalculable.” Now the nation hurtles toward a milestone of 1 million. What is 10 times incalculable?
And it just keeps going from there — this is one of those articles so well written and packed with so much information and insight that it’s difficult not to quote the whole thing, even though it paints a bleak picture of America. Read the whole thing here. See also Yong’s accompanying Twitter thread.
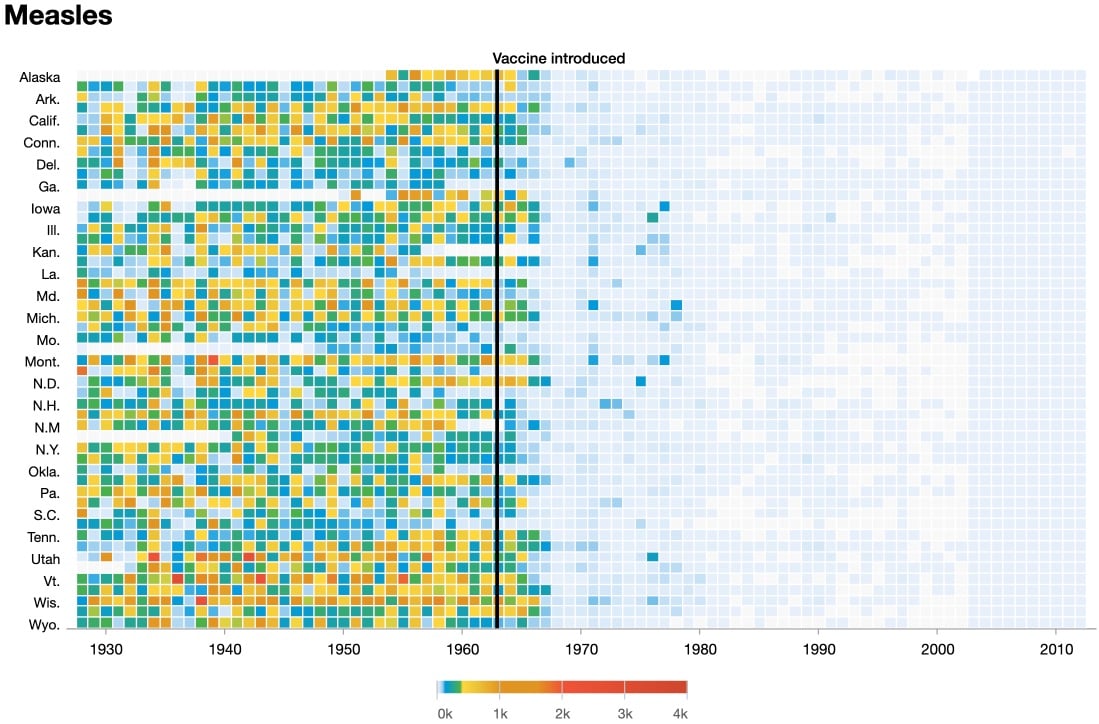
Historically, contracting the measles has been linked to subsequent illness (and possibly death) from other causes. In the past few years, scientists have discovered why this is: measles causes “immune amnesia”.
Enter “immune amnesia”, a mysterious phenomenon that’s been with us for millennia, though it was only discovered in 2012. Essentially, when you’re infected with measles, your immune system abruptly forgets every pathogen it’s ever encountered before — every cold, every bout of flu, every exposure to bacteria or viruses in the environment, every vaccination. The loss is near-total and permanent. Once the measles infection is over, current evidence suggests that your body has to re-learn what’s good and what’s bad almost from scratch.
“In a way, infection of the measles virus basically sets the immune system to default mode,” says Mansour Haeryfar, a professor of immunology at Western University, Canada, “as if it has never encountered any microbes in the past”.
This re-learning process takes up to three years, which “around the time it takes infants to acquire immunity to everyday pathogens in the first place”. In the meantime…
It’s not surprising, then, that measles doesn’t just increase the risk of illness, but also death. In fact, childhood mortality from other viruses is strongly linked to the incidence of measles. The 2015 study showed that when childhood mortality in the UK, US, or Denmark goes up, this is usually because measles has become more prevalent.
The findings explain why vaccinating children against measles has the unexpected, beneficial side-effect of reducing deaths among children, way beyond the numbers who were ever at risk of dying from measles itself.
Of course, an extremely effective and safe vaccine offers protection against both measles and the immune amnesia it causes. But with the steep rise in anti-vaccination sentiment during the pandemic and the increasing willingness of conservative leaders to disregard public health protections in favor of “individual freedom”, widely vaccinating against this dangerous pathogen in the US & elsewhere will be more difficult than in the past.
Older posts
Socials & More